D5 a Ns 1ml Continuous Infusion
Fluid and Electrolyte Therapy
A Chapter in Core Concepts of Pediatrics, 2nd Edition
Fluid and Electrolyte Therapy
Marie Dawlett MD and Amy Gonzalez MD
The Need for Water
 We drink water, or a water-containing beverage, five to ten times a day. We do not have to keep track of our fluid intake.
We drink water, or a water-containing beverage, five to ten times a day. We do not have to keep track of our fluid intake.
The thirst-creating mechanism is exquisitely sensitive to an increase in plasma osmolality and as long as there is free access to water, intake will never be less than the need.
So, we rely on thirst to guide water intake. But what about a person who is receiving only intravenous fluids or gavage feeding? In this individual, the thirst mechanism has been bypassed. You, the prescribing physician, must decide how much fluid to administer. Maintenance fluids are necessary to maintain homeostasis when a patient is unable to intake the required water and should be prescribed, ordered, dosed, and delivered like any other drug.
So how much water does a person need in a day? To answer this question, we must ask another.
The only absolute reason to drink water is to replace losses. The need for water over any period of time is equal to the loss of water over that period of time. Conventionally, water requirement is calculated in daily, or 24-hour, increments.
To be able to calculate daily water requirement, we need to be able to estimate daily water loss in individuals of different ages. For this, we need to know the routes of water loss and be familiar with the physiologic and pathological determinants of the rate of loss from each route.
Photo by Konstantin Tavrov from Photospin
Routes of Water Loss
Water loss from the body is said to be either "sensible" or "insensible". You must have heard these terms before. What do they mean?
"Sensible" loss is loss that can be perceived by the senses and can be measured. If you've lost it, you know you've lost it!
"Insensible" losses can neither be perceived nor measured directly. You've lost it, but you don't know that you've lost it (and, of course, you do not know how much you have lost...)
Urine, of course is a "sensible" loss - it can be seen, felt, and measured!
Respiratory loss is an insensible loss. This is water that is used to humidify inspired air and is then breathed out as water vapor. What is the other major insensible route of water loss? Check out the cards below. Note: water loss in normal stool is inconsequential.
Determinants of water loss
- Respiratory water loss is a function of the amount of air that is moved in and out of the lungs, or breathed, per unit time. Unless the ambient relative humidity is 100%, this air needs to be humidified, and the water used for humidification is breathed out.
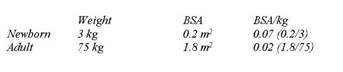
- The amount of air breathed depends on oxygen need and carbon dioxide production, which in turn depend on the metabolic rate (MR). The MR does not rise linearly with increase in body weight. MR/kg is highest in newborns and lowest in adults. Respiratory water loss/kg follows the same pattern.
- Transcutaneous evaporative water loss depends on body surface area (BSA). The BSA/kg body weight is highest in newborns and lowest in adults. Transcutaneous evaporative water loss/kg follows the same pattern.
Of course, these statements assume normal body temperature and identical ambient temperature and humidity.
| More info: Determinants of water loss |
| 1. Respiratory losses are dependent on the respiratory rate (RR) and tidal volume. Unless the ambient humidity is 100%, inspired air has to be humidified. The RR for a newborn is about 40/min. Wth a weight of 3 kg and a tidal volume of 6 ml/kg, the minute ventilation is 40 breaths/min X 3kg X 6 ml/breath*kg = 720 ml/min, or 240 ml/kg/min. RR for an adult is 12/min. Assuming weight of 70 kg and a tidal volume of 6 ml/kg, minute ventilation for an adult is 12 breaths/min X 70 kg X 6 ml/breath*kg = 5040 ml/min or 72 ml/kg/min. As can be seen, a newborn uses, and therefore has to humidify, 3.5 times as much air every minute as an adult. As a child grows, minute ventilation does not rise in direct proportion to the weight so neither does lung water loss. 2. Transcutaneous evaporative water loss is dependent on body surface area (BSA). A newborn has almost 4 times as much BSA/kg as an adult, so transcutaneous evaporative water losses are proportionately higher. As the child grows, BSA/kg does not rise in direct proportion to the weight, so neither does transcutaneous evaporative water loss. In summary, the water loss per kg body weight from these two routes is highest in the newborn. As the child grows, the increase in the rate of water loss is less than the increase in weight. |
- Obligatory urine volume depends on the amount of waste solute that needs to be excreted and the ability to concentrate the urine. Urinary solutes are derived largely from ingested protein and electrolytes. The intake of these substances is higher in younger children than in adults. In addition, young infants cannot concentrate urine to the same extent as older children. For these reasons, obligatory urine output is higher in infants and children as compared to adults.
Putting it all together, the rate of water loss from all three routes is highest in the smallest children and does not rise in direct proportion to increase in body weight.
Normal Maintenance Requirements
It is clinically useful to begin fluid therapy by estimating normal maintenance requirements using the estimated caloric expenditure method. The resting energy expenditure in healthy children is vastly different from those with an acute disease and/or illness or after surgery.
The commonly used method for approximating water loss (and therefore the water requirement) is based off of the Holliday-Segar nomogram. This formula is based on the energy expenditure of healthy children, with 1 mL of fluid provided for each kcal expended, or 1500 mL/m2 per day.
Holliday and Segar collated information from a number of studies, including their own, and concluded the following:
- Water loss (and therefore water requirement) is a function of caloric expenditure.
- Total daily water requirement to replace insensible and urinary water loss in the hospitalized patient is approximately 100 ml/100kcal/day. This means that for every 100 kcal burned, the patient utilizes 100 ml of fluid.
- Caloric expenditure, and therefore the water requirement, for the hospitalized patient can be estimated from the nomogram shown below.
The diagram below is taken from their original publication "The maintenance need for water in parenteral fluid therapy", Pediatrics 1957. Holliday and Segar determined how many calories a patient burns as a factor of weight.
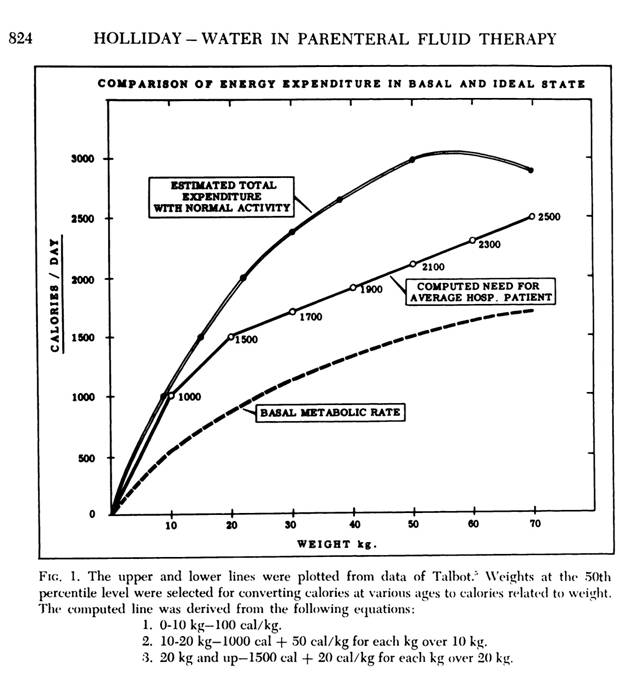
Holliday MA and Segar WE. p. 823-8232, Pediatrics 1957
The Holliday-Segar nomogram approximates daily fluid loss, and therefore the daily fluid requirements, as follows:
- 100 ml/kg for the 1st 10 kg of wt.
- 50 ml/kg for the 2nd 10 kg of wt.
- 20 ml/kg for the remaining wt.
Even though it is correct to think about fluid requirements on a 24-hour basis, the delivery pumps used in hospitals are designed to be programmed for an hourly infusion rate. The 24-hour number is often divided into approximate hourly rates for convenience, leading to the "4-2-1" formula.
- 100 ml/kg/24-hours = 4 ml/kg/hr for the 1st 10 kg
- 50 ml/kg/24-hours = 2 ml/kg/hr for the 2nd 10 kg
- 20 ml/kg/24-hours = 1 ml/kg/hr for the remainder
Quickchecks
Calculate the maintenance water required for a 17kg child? Click here for the answer.
Calculate the maintenance water required for 30 kg child? Click here for the answer.
Sodium and Potassium Requirements
Quickcheck
It is clear that there is no strict daily sodium requirement since, in the normal individual, homeostatic mechanisms will instruct the kidney to conserve or excrete sodium and keep total body sodium content within the normal range.
| More info: The Consequences of Pizza |
| Salt intake ==> increase in plasma Na and osmolality ==> increased thirst and increased ADH secretion ==> chug-a-lug ==> water intake and water retention, plasma dilution ==> plasma Na and osmolality decline almost to baseline at the expense of expanded plasma volume (I cannot take off my rings; socks leave deep marks on shin!) ==> the kidney stops making renin ==> no renin, so no angiotensin and no aldosterone ==> Na re absorption declines in the collecting duct ==> urinary Na excretion increases until all the salt from the pizza has been excreted ==> plasma osmolality falls as Na is excreted ==> ADH shuts off ==> water is excreted until plasma volume has declined to baseline... I feel better. Whew! |
Based on recommendations made by Holliday and Segar, the daily sodium requirement was estimated at 3 mEq/100 ml of water water requirement. Holliday and Segar decided on this number by looking at the sodium content of human and cows' milk. So, Na is added to maintenance fluids at a concentration of 3 mEq/100ml or 30 mEq/L. For an adult, this will provide about 75 mEq of Na/day, equivalent to approximately 4.5 G of salt. Click for flashback to chemistry.
When we speak about adding sodium to IV fluids, we talk about it in terms of normal saline. Normal saline is isotonic to plasma. Normal saline is 154 mEq/L. So if we wanted to add 30mEq/L of Na, we would need 1/5NS. (154 mEq/L divided by 5 is roughly 30 mEq/L).
For decades, our maintenance IV fluids have ranged anywhere from 1/5NS to 1/3NS to Ѕ NS. Note that all of these are considered hypotonic to plasma. Based on current research, it is determined that giving hypotonic solutions as maintenance IV fluids is associated with severe morbidity and even mortality due to hyponatremia.
reference: AAP Guidelines on Maintenance IV Fluids in Hospitalized Children
We know that kids in the hospital are stressed. They are vomiting, or have respiratory illness, or require surgery, or have fever. All of these things cause an increase in ADH release. The more ADH, the more water is reabsorbed from the collecting duct of the kidneys. Combine this with hypotonic IV fluids, and you have a perfect formula for hyponatremia.
The maintenance K requirement is estimated at 2 mEq/100 ml of fluid or 20 mEq/L. Potassium either comes pre-added or can be manually added to any intravenous solution at a concentration of 2 mEq/100 ml or 20 mEq/L to provide the appropriate amount of K for maintenance. This was estimated by Holliday and Segar to again reflect the composition of human and cow milk and has remained the same since then.
In children who have a condition that might predispose to renal failure, such as dehydration, K is not added to intravenous fluids until the presence of renal function has been established.
Note: K concentration in IV fluids of up to 40 mEq/L is used for correction of hypokalemia. A concentration exceeding 40 mEq/L is irritating to the veins and may be dangerous!
Common Crystalloid Intravenous Fluids
| More Info: normal saline |
| • Normal saline is 0.9% saline. This means that there is 0.9 G of salt (NaCl) per 100 ml of solution, or 9 G per liter. • This solution has 154 mEq of Na per liter. In fact, all the other solutions listed on the previous screen will be compared to normal saline as if it has 150 mEq of Na/L. • This solution is used for correction of hypovolemia. • This solution is used for maintenance IV fluids in all pediatric patients greater than 1 month old due to the risk of hyponatremia with hypotonic IV fluids. • Useful hint: if you ever have to convert grams of salt (NaCl) into mEq of Na, just remember normal saline: 9G of salt = 154 mEq of Na. You can apply this conversion factor to any other amount. |
| More info: D5 0.50% normal saline |
| You will notice that all solutions that have less salt than normal saline have 5% dextrose added to them. There are two reasons for this: • Normal saline has an osmolality close to that of plasma. Any solution that has less salt will be hypo-osmolar. Rapid infusion of a hypo-osmolar solution can cause osmotically induced water shift into the cells, and this can lead to detrimental effects such as hemolysis. Addition of 5% dextrose ensures that the infused solution will have an osmolality equal to or higher than plasma regardless of the salt concentration. • A 5% dextrose solution provides at least some calories to a person who might have no other nutritional intake and will reduce catabolism. |
| More info: Ringer's Lactate (LR) | |||||||||||||||||||||
| Ringer's lactate (LR) is a composite fluid that is available with and without dextrose.
The lactate is metabolized in the liver to bicarbonate. LR provides a source of base, as well as some Ca. LR is not often used by pediatricians in the US. |
Maintenance Fluid Requirements in Disease
Maintenance fluid calculations assume that fluid loss from sensible and insensible routes is taking place at a normal rate. But a febrile infant will be having a much greater transcutaneous evaporative water loss than one with a normal body temperature. Similarly, a child with tachypnea will lose excess water from the lungs - unless she is receiving humidified oxygen, in which case she will lose none!
Also consider patients with kidney disease who have anuria, oliguria, or polyuria. Maintenance IV fluids for these patients will not be written with the standard formula because their urinary losses are not taking place at a normal rate. Maintenance fluids using the standard formula would be too much for an anuric child with no urinary losses and too little for those with a concentrating defect in their kidneys causing polyuria.
Important: Before using a standard formula for calculating maintenance fluids, ensure that the child is not having higher or lower losses than usual!
As a rule of thumb, total water loss can normally be broken down as follows:
For a 10 kg child (water loss: 1000 ml/day), loss from the different routes for a 24-hour period would be:
When we prescribe maintenance fluid for a 10 kg child for 24 hours as 1000 ml, we are assuming that loss from the various routes is occurring at a normal rate. However, adjustments are sometimes necessary:
- Tachypnea: Add 20-50% to the respiratory replacement. Note: If a person is receiving humidified oxygen, respiratory water loss is nil.
- Fever: Add 10% to the transcutaneous loss replacement for every degree temperature above 38o C.
- Anuria: Exclude urinary loss from replacement.
- Oliguria: Measure actual urine output every 12 hours and add it to the insensible loss for the next 12 hours.
- Polyuria: Measure actual urine output every 1-2 hours and add it to the insensible loss for the next 1-2 hours.
What is the 24-hour fluid requirement for a 10 kg child who has a fever of 40 degrees C. and a respiratory rate of 70/min? (Presuming the child is not receiving humidified O2)
What volume of maintenance fluid would you order for the next 12 hours for a 10 kg child with oliguria whose measured urine output in the previous 12 hours has been 50 ml?
Dehydration in Children
 In children, the most common cause of dehydration is diarrheal fluid loss. In the majority of children with dehydration secondary to gastrointestinal loss, the serum sodium level is within the normal range (135-145 mEq/L). This is known as isotonic dehydration.
In children, the most common cause of dehydration is diarrheal fluid loss. In the majority of children with dehydration secondary to gastrointestinal loss, the serum sodium level is within the normal range (135-145 mEq/L). This is known as isotonic dehydration.
Electrolyte losses from diarrhea and vomiting range from iso- to hypo- osmolar. The tendency to have hypernatremia from loss of hypo-osmolar fluid is partially countered by movement of fluid from the ICF to the ECF driven by the increase in ECF osmolality. This also helps maintain intra vascular volume.
Hyponatremic (hypotonic) dehydration (serum sodium concentration < 135 mEq/L) indicates body water content in excess of sodium content. One potential scenario for hyponatremic dehydration is replacement of fluid loss by electrolyte-free water such as apple juice or iced tea, or with hypotonic fluids such as D5 0.20% saline (fifth-normal saline). Because of anti-diuretic hormone (ADH) secretion stimulated by hypovolemia, water will be retained even in the face of a falling serum sodium level.
Hypernatremic (hypertonic) dehydration (serum sodium concentration
> 145 mEq/L) indicates excessive free water loss. For example, a child who is on gavage feeding with a fixed daily fluid intake and develops excessive fluid loss from tachypnea or fever will gradually develop hypernatremia. Hypernatremia is also seen in a small proportion of children with gastroenteritis and dehydration, presumably from excessive loss of water in relation to solute.
Photo by lev dolgachov from Photospin
Clinical Assessment of Dehydration
Clinical assessment of dehydration is always approximate, and the child should be frequently re-evaluated for continuing improvement during correction of dehydration.
When we talk of "5% dehydration", it means that the child has lost an amount of fluid equal to 5% of the body weight. If you have an accurate pre-illness weight, you may use that weight. Alternatively, the pre-illness weight can be calculated as follows:

So,
- A 10 kg child who is 5% dehydrated will weigh 9.5 kg.
- A 10 kg child who is 10% dehydrated will weigh 9 kg.
- A 5 kg child who is 10% dehydrated will weigh 4.5 kg.
The child's current (dehydrated) weight can be used for calculation of dehydration and maintenance fluids. After all, clinical assessment of dehydration, and therefore the volume needed for correction, is approximate!
Replacement Fluid Therapy
 The initial goal of treating dehydration is to restore intravascular volume (resuscitative phase). The simplest approach is to replace dehydration losses with 0.9% saline. This ensures that the administered fluid remains in the extracellular (intravascular) compartment, where it will do the most good to support blood pressure and peripheral perfusion.
The initial goal of treating dehydration is to restore intravascular volume (resuscitative phase). The simplest approach is to replace dehydration losses with 0.9% saline. This ensures that the administered fluid remains in the extracellular (intravascular) compartment, where it will do the most good to support blood pressure and peripheral perfusion.
Therapy may be started with a rapid bolus of 0.9% saline to combat incipient shock. But correction of dehydration must be accompanied by provision of maintenance fluid. After all, the child is breathing, losing free water through the skin, and is urinating! As discussed earlier, maintenance fluid is provided as D5NS.
A typical sequence of events in the management of a child with 10% dehydration AND A NORMAL SERUM SODIUM LEVEL is given below. Management of children with a serum sodium level of < 135 or> 145 mEq/L is beyond the scope of this discussion.
Step 1: In the ER, the child is estimated as having 10% dehydration. The blood pressure is low and the heart rate is very high. This child is in shock. The goal is to rapidly stabilize the vital signs; maintenance fluid is not a consideration at this time.
The child is given a 20 ml/kg bolus of 0.9% saline over 10-20 minutes. The vital signs stabilize (the bolus can be repeated if necessary).
Step 2: The patient is transferred to the inpatient unit. By this time, serum electrolyte levels are available and the serum sodium concentration is within the normal range. Subsequent fluid therapy is calculated as follows:
This child's total fluid loss was 10% of 10 kg, or 1000 ml. Of this, 200 ml has already been infused in the ER, so the remaining deficit is 800 ml.
Typically, half the total deficit is replaced in the first eight hours after admission and the remaining fluid is given over the next 16 hours. So, this child needs 300 ml of NS in the next eight hours (for a total of 500 ml) and another 500 ml in the next 16 hours.
However, maintenance fluid must also be administered. The volume of maintenance fluid for 24 hours is 1000 ml (100 ml/kg X 10 kg). This needs to be given as D5NS, with our without potassium, depending on the patient's urine output. If the child is not urinating well, hold on adding potassium.
Note #1: Once the child has started urinating, KCl should be added to the intravenous fluids at a concentration of 20 mEq/L.
Note #2: If the child continues to vomit or have significant diarrhea, the volume of ongoing fluid loss should be estimated and added to the deficit every few hours as 0.9% saline. Ideally, the diapers should be weighed. If this is not possible, then a volume of 50-100 ml should be used for each stool in an infant and 100-200 ml for the older child.
Note #3: The dehydration component of fluid replacement MUST be provided as 0.9% saline. NEVER use a hypotonic saline, such as D5 0.18% (fifth-normal saline), D5 0.3% (third-normal saline) or even D5 0.45% (half-normal saline) to correct dehydration. Dehydration and hypovolemia result in secretion of anti-diuretic hormone, which causes retention of free water, and provision of hypotonic replacement fluid can lead to potentially life-threatening hyponatremia.
Step 3: Suppose the child is well hydrated by the second hospital day, but is still feeling queasy and does not want to drink. Maintenance fluids can now be continued as D5 NS with 20 mEq/L of KCl.
Important
- If you are correcting only dehydration (as when giving a bolus in the ER), use 0.9% saline.
- If you are providing fluid only, may use D5NS with 20 mEq/L KCl.
- Estimate and replace ongoing losses, if significant.
| More info: hypernatremia and hyponatremia |
| The blood brain barrier prevents rapid movement of solutes out of or into the brain. On the other hand, water can move freely across the blood brain barrier. Rapidly developing hyponatremia causes a shift of water into the brain; conversely, hypernatremia can lead to brain dehydration and shrinkage. Severe, acute hyponatremia may result in brain edema with neurological symptoms such as a change in sensorium, seizures, and respiratory arrest. This is a life-threatening medical emergency and requires infusion of hypertonic saline. Acute hypernatremia results in a reduction in brain volume. This can lead to subdural bleeding from stretching and rupture of the bridging veins that extend from the dura to the surface of the brain. Given time, the brain can alter intracellular osmotic pressure to better match plasma osmolality. With persistent or slowly developing hyponatremia, brain cells extrude electrolytes and organic osmoles and the increase in brain volume is blunted or avoided. Neurologic symptoms are absent or subtle. With persistent hypernatremia, brain cells generate organic osmoles (also known as idiogenic osmoles) to compensate for the increase in plasma osmolality. Again, the change in brain volume is partially blunted. These processes take 24-48 hours to become effective and leave the brain with a decreased (in hyponatremia) or increased (hypernatremia) osmolar content. Just as the adaptation takes 24 hours or more, un-adaptation also takes time. Rapid correction of long-standing hypo- or hypernatremia has the potential for severe neurological consequences because of sudden changes in brain volume in the opposite direction. The neurologic manifestations associated with overly rapid correction of hyponatremia is called osmotic demyelination syndrome. Thus, hyper- or hyponatremia of long duration should be corrected slowly. |
Photo by Javier Correa from Photospin
Oral Rehydration Therapy
Over the past four decades, oral rehydration has been demonstrated to be quite effective in replacing diarrheal fluid losses. This therapy is best reserved for the child with mild or moderate dehydration.
The intestine (both the small bowel and colon) is remarkably efficient in its ability to absorb water. The small bowel absorbs the vast majority of the body's fluid needs.
Oral Rehydration Therapy (ORT) is accepted as the standard of care and first line treatment for the management of acute gastroenteritis with or without mild to moderate dehydration.
The following properties for ORT are recommended by the World Health Organization (WHO)
- Total osmolality between 200 and 310 mOsm/L
- Equimolar concentrations of glucose and sodium
- Glucose concentration <20 g/L (111 mmol/L)
- Sodium concentration between 60 and 90 mEq/L
- Potassium concentration between 15 and 25 mEq/L
- Citrate concentration between 8 and 12 mmol/L
- Chloride concentration between 50 and 80 mEq/L
There are commercially available preparations that approximate these concentrations such as Pedialyte®, Enfalyte®, and Rehydralyte®.
Note: Patients with mild to moderate dehydration can be treated with ORT. Those with severe dehydration are not candidates and need IV infusions. Also, those patients with altered mental status who may be at risk for aspiration and those patients with intestinal diseases such as short gut or ileus are also not candidates. Vomiting is not a contraindication for ORT.
Phases of Oral Rehydration Therapy
ORT encompasses two phases of treatment
- Rehydration phase. Water and electrolytes are administered as oral rehydration solution (ORS) to replace existing losses (the deficit is replaced quickly over 3-4 hours)
- Maintenance phase: This includes both replacement of ongoing fluid and electrolyte losses and adequate dietary intake.
During both phases, fluid losses from vomiting and diarrhea are replaced in an ongoing manner. An age-appropriate, unrestricted diet should also be instituted after the dehydration is corrected. If the patient is breastfed, breastfeeding should continue during this phase as well as during the maintenance phase. Formula-fed infants should continue their usual formula immediately upon rehydration. Lactose-free or lactose-reduced formulas usually are unnecessary. The BRAT (banana-rice-applesauce-toast) diet is unnecessarily restrictive and can provide suboptimal nutrition.
How to Administer Oral Rehydration Therapy
ORS is administered in frequent, small amounts of fluid by spoon or syringe. A nasogastric tube can be used in the child who refuses to drink. Nasogastric (NG) feeding allows continuous administration of ORS at a slow, steady rate for patients with persistent vomiting. For those with vomiting, the majority can be rehydrated successfully with oral fluids if limited volumes of ORS (5 mL) are administered every 5 minutes, with a gradual increase in the amount consumed.
Mild to Moderate Dehydration
Rehydration phase: the dose is 50-100 ml/kg over 3-4 hours.
During both phases, ongoing losses from diarrhea and vomiting are replaced with ORS. If the losses can be measured accurately, 1 mL of ORS should be administered for each gram of diarrheal stool. Alternatively, 10 mL/kg of body weight of ORS should be administered for each watery or loose stool, and 2 mL/kg of body weight for each episode of emesis.
Severe Dehydration
Severe dehydration is a medical emergency, and requires emergent IV therapy with rapid infusion of 20 mL/kg of isotonic saline. As the patient's condition improves, therapy can be later changed to ORT.
Now let's practice
Source: https://www.utmb.edu/pedi_ed/corev2/fluids/Fluids_print.html
0 Response to "D5 a Ns 1ml Continuous Infusion"
Post a Comment